
Sleep is as essential to health as food and water. Yet for millions of people, quality sleep remains frustratingly out of reach. Understanding insomnia—what it is, why it happens, and how to treat it—can make the difference between suffering in silence and reclaiming restorative rest.
What Is Insomnia?
Insomnia is defined as persistent difficulty falling asleep, staying asleep, or waking too early, despite having adequate opportunity to sleep. To meet diagnostic criteria, these sleep difficulties must occur at least three nights per week for at least three months and must cause significant distress or impairment in daily functioning.
Insomnia isn’t just about the quantity of sleep—it’s about quality and the impact on daytime life. People with insomnia often report fatigue, difficulty concentrating, mood disturbances, and decreased performance at work or school, even when they’ve spent adequate time in bed.
The Architecture of Sleep
To understand what goes wrong in insomnia, it helps to understand normal sleep. Sleep isn’t a uniform state—it’s a dynamic process cycling through distinct stages, each serving different biological functions.
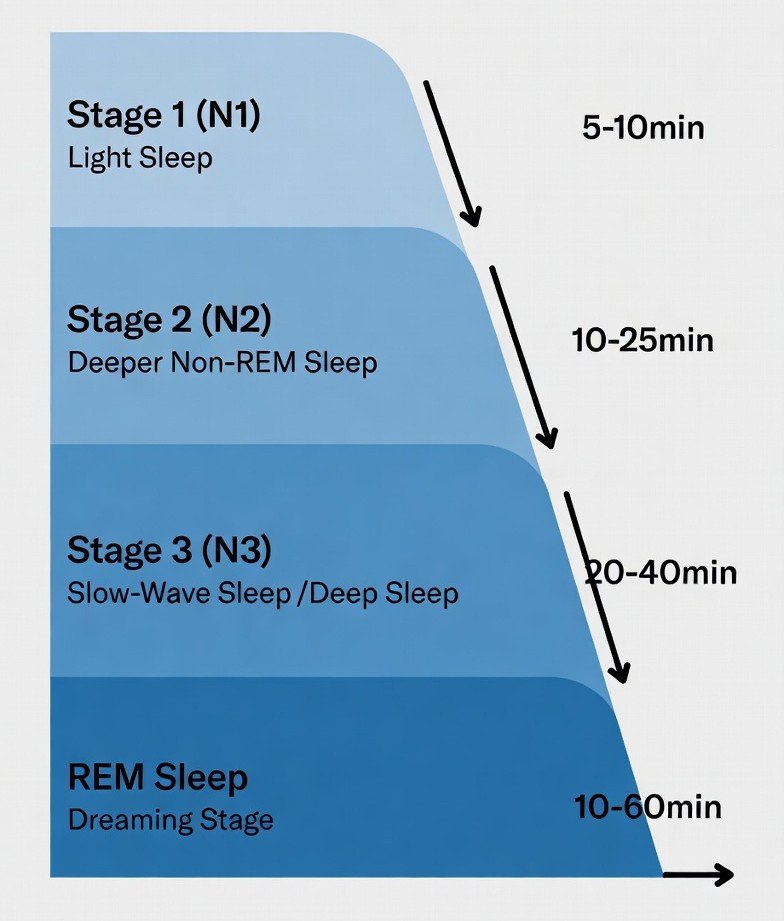
Stage 1 (N1): The transition from wakefulness to sleep. Easily disrupted, lasting only a few minutes.
Stage 2 (N2): Light sleep where body temperature drops and heart rate slows. Makes up about 50% of total sleep.
Stage 3 (N3): Deep, slow-wave sleep critical for physical restoration, immune function, and memory consolidation. Hardest to wake from.
REM Sleep: Rapid Eye Movement sleep, where most vivid dreaming occurs. Essential for emotional processing, learning, and memory.
Throughout the night, these stages repeat, with deep sleep (N3) dominating early cycles and REM sleep increasing toward morning. Sleep Cycle is approximately 90 minutes per cycle, 4-6 cycles per night. Disruption of any stage—particularly deep sleep and REM sleep—can leave you feeling unrefreshed, even if total sleep time seems adequate.
What Causes Insomnia?
• Medical Conditions: Chronic pain, respiratory disorders (like sleep apnea), restless leg syndrome, hormonal changes, and neurological conditions
• Stress and Anxiety: Racing thoughts, worry, and hyperarousal prevent the relaxation necessary for sleep onset
• Depression: Both insomnia and hypersomnia are core features of depression; early morning awakening is particularly common
• Poor Sleep Hygiene: Irregular sleep schedules, excessive screen time before bed, uncomfortable sleep environment
• Medications: Stimulants, corticosteroids, some antidepressants, beta-blockers, and decongestants can interfere with sleep
• Circadian Rhythm Disorders: Shift work, jet lag, delayed sleep phase syndrome
• Substance Use: Caffeine, nicotine, alcohol (which fragments sleep architecture despite initial sedation), and stimulant drugs
Insomnia is rarely a standalone problem. It typically arises from an interplay of biological, psychological, and environmental factors.
Primary Contributors:
In many cases, insomnia becomes self-perpetuating—worry about not sleeping creates anxiety that further disrupts sleep, creating a vicious cycle.

The Mental Health Toll of Poor Sleep
The relationship between sleep and mental health is bidirectional. Mental health disorders can cause insomnia, and chronic insomnia significantly increases the risk of developing psychiatric conditions.
Cognitive Impacts:
- Memory consolidation deficits
- Impaired concentration, attention, and decision-making
- Impaired concentration, attention, and decision-making
- Slowed reaction time and processing speed
- Reduced executive function
Emotional Impacts:
- Higher risk of developing depression and anxiety disorders
- Increased suicidal ideation in severe cases
- Increased irritability and emotional reactivity
- Difficulty regulating emotions
Neurobiological Changes: Chronic sleep deprivation alters brain function, particularly in the prefrontal cortex (responsible for executive control) and amygdala (involved in emotional processing). This creates a neurological vulnerability to mood disorders.
Longitudinal studies show that persistent insomnia doubles the risk of developing major depression, even after controlling for other risk factors. The message is clear: treating sleep problems is not just about rest—it’s about protecting long-term mental health.
Treatment Options: What Actually Works
Effective insomnia treatment typically combines behavioral interventions with, when necessary, short-term pharmacological support.
Behavioral Treatments (First-Line Approach)
Cognitive Behavioral Therapy for Insomnia (CBT-I) is the gold standard treatment, backed by extensive research. It’s as effective as medication in the short term and more effective long-term, with benefits persisting years after treatment ends.

CBT-I typically includes:
• Sleep Restriction: Limiting time in bed to match actual sleep time, then gradually increasing it—paradoxically improves sleep efficiency
• Stimulus Control: Reassociating the bed with sleep by using it only for sleep and sex, not for scrolling, watching TV, or worrying
• Cognitive Restructuring: Addressing dysfunctional beliefs and anxiety about sleep
• Sleep Hygiene Education: Optimizing environment and habits
• Relaxation Techniques: Progressive muscle relaxation, diaphragmatic breathing, mindfulness
Other behavioral approaches include light therapy for circadian rhythm disorders and biofeedback.

Medication Options
When behavioral approaches alone are insufficient, medications may provide short-term relief. However, they should ideally be used as a bridge while implementing behavioral strategies, not as a permanent solution.
Z-Drugs (Zolpidem, Eszopiclone, Zaleplon):
- Modern sleep aids that target specific GABA receptors
- Shorter half-lives than older benzodiazepines, reducing next-day sedation
- Concerns: Complex sleep behaviors (sleepwalking, sleep-eating), tolerance, rebound insomnia upon discontinuation
- Best for: Short-term use (typically 2-4 weeks)
Benzodiazepines (Temazepam, Lorazepam):
- Effective for sleep induction but reduce deep sleep quality
- Long-acting formulations (like temazepam) may help with sleep maintenance but risk next-day impairment
- Concerns: High potential for dependence, tolerance, cognitive impairment, increased fall risk (especially in elderly), rebound insomnia
- Generally not recommended for long-term use
Sedating Antidepressants (Trazodone, Mirtazapine, Doxepin):
- Often prescribed off-label for insomnia, particularly when depression is also present
- Trazodone (50-100mg) is widely used; low doses of doxepin (3-6mg) are FDA-approved for sleep maintenance
- Side effects: Morning grogginess, weight gain (mirtazapine), orthostatic hypotension (trazodone)
- May be reasonable for long-term use when depression coexists
Sedating Antipsychotics (Quetiapine, Olanzapine):
- Sometimes prescribed off-label at low doses for treatment-resistant insomnia
- Concerns: Significant side effects including metabolic changes (weight gain, diabetes risk), extrapyramidal symptoms, and limited evidence for efficacy in primary insomnia
- Should generally be reserved for cases where insomnia coexists with bipolar disorder, psychotic disorders, or severe treatment-resistant cases
- Not recommended as first-line agents due to unfavorable risk-benefit ratio
Antihistamines (Diphenhydramine, Doxylamine):
- Available over-the-counter; induce drowsiness by blocking histamine receptors
- Less ideal due to: Rapid tolerance development, anticholinergic side effects (dry mouth, constipation, urinary retention, confusion—especially problematic in elderly), next-day sedation, cognitive impairment
- Not recommended for chronic use
Melatonin and Melatonin Receptor Agonists (Ramelteon):
- Melatonin: Supplements can help with circadian rhythm disorders and jet lag; evidence for primary insomnia is mixed
- Ramelteon: FDA-approved prescription melatonin receptor agonist; minimal side effects, no abuse potentiBest for: Circadian rhythm disorders, sleep onset difficulties
Orexin Receptor Antagonists (Suvorexant, Lemborexant):
- Newer class that blocks wakefulness signals rather than promoting sedation
- Lower risk of dependence and tolerance compared to benzodiazepines
- Side effects: Next-day somnolence, sleep paralysis, complex sleep behaviors (rare)
- Emerging as potentially safer long-term options
The Bottom Line
Insomnia is a treatable condition, but treatment requires more than just a pill. The most effective approach combines:
1. Behavioral interventions first (especially CBT-I)
2. Addressing underlying causes (medical, psychiatric, environmental)
3. Judicious, short-term use of medication when necessary to break severe cycles
4. Gradual tapering of medications while reinforcing behavioral strategies
If you’re struggling with sleep, start by tracking your patterns, optimizing your sleep environment, and considering a referral to a sleep specialist or therapist trained in CBT-I. Quality sleep is foundational to mental and physical health—and with the right approach, it’s within reach.
________________________________________
Resources:
• American Academy of Sleep Medicine: www.sleepeducation.org
• National Sleep Foundation: www.sleepfoundation.org
• CBT-I Provider Directory: www.behavioralsleep.org
References:
• Morin, C. M., et al. (2015). Cognitive behavioral therapy for chronic insomnia: A systematic review and meta-analysis. Annals of Internal Medicine, 163(3), 191-204.
• Riemann, D., et al. (2017). European guideline for the diagnosis and treatment of insomnia. Journal of Sleep Research, 26(6), 675-700.
• Krystal, A. D., et al. (2019). The assessment and management of insomnia: An update. World Psychiatry, 18(3), 337-352.
• Sateia, M. J., et al. (2017). Clinical practice guideline for the pharmacologic treatment of chronic insomnia in adults: An American Academy of Sleep Medicine clinical practice guideline. Journal of Clinical Sleep Medicine, 13(2), 307-349.




